
Pipet Curet




The Pipet Curet™ is a gold standard, single-use, sterile, disposable, suction curette for obtaining a histologic biopsy of the uterine mucosal lining or sample extraction of uterine menstrual content for microscopic examination or culturing.
- Description
- Specifications
- Catalogue
- Media
Pipet's intuitive design provides consistency of sample collection every time. The procedure takes less than a minute to perform and produces little if any post-procedure bleeding or patient discomfort. Completely self-contained, the Pipet Curet™ requires no additional equipment to complete the procedure. In most cases, the Pipet Curet™ can be inserted without the need for dilation. Curette flexibility has been optimized to facilitate adaptation to normal uterine curvature, thus promoting contact with the wall for safe, improved sample collection.

WARNINGS
- In patients with amenorrhea, obtaining an endometrial biopsy with the Pipet Curet™ should be performed only after confirmation of the absence of detectable circulating HCG levels.
- Contents supplied sterile. Do not use if sterile barrier is damaged.
- For single use only. Do not reuse, reprocess or resterilize. Reuse, reprocessing or resterilization may compromise the structural integrity of the device and/or lead to device failure which, in turn, may result in patient injury, illness or death. Reuse, reprocessing or resterilization may also create a risk of contamination of the device and/or cause patient infection or cross infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device may lead to injury, illness or death of the patient. Dispose of in accordance with all applicable Federal, State and local Medical/Hazardous waste practices.
INDICATIONS FOR USE
Histologic biopsy of the epithelium and glandular mucosal layer (endometrium) of the uterine wall or sample extraction of uterine menstrual content for:
- Detection of endometrial carcinoma and precancerous conditions
- Determination of endometrial tissue response to hormonal influences by visual observation of the histologic sample, such as:
a. Endometrial dating
b. Periodic scrutiny of the effects of hormonal therapy on the uterine endometrium, particularly in patients receiving estrogen replacement therapy for menopausal symptoms and prophylaxis of osteoporosis
c. Luteal insufficiency (visually determined histologically from endometrial tissue obtained only during the secretory [pro gestational] phase of the menstrual cycle)
d. Functional metrorrhagia (contraception, pre-menopause) - Diagnosis of pathology associated with infertility
- Bacterial culturing to specifically identify causative uterine pathogens
CONTRAINDICATIONS
- Patients where pregnancy is suspected
- Patients with, or recently recovered from pelvic inflammatory disease
- Patients with any cervical or pelvic infections (infections should be treated and cured before performing any endometrial sampling procedure)
- Patients suffering from any diseases or conditions which could under all circumstances contraindicate outpatient surgical treatment, e.g., severe anemia, heart disease, or clotting mechanism deficiencies
In general, the same criteria for regular hospital D&C should be followed for office suction curettage.
PRECAUTIONS
By virtue of its flexibility and small caliber, with the Pipet Curet™ a histologic endometrial biopsy can be performed with minimal danger of uterine wall perforation. However, care should be taken prior to its insertion to ascertain the depth of the uterus and any uterine retroflexion or anteflexion present in individual patients. Best clinical judgement should be used to allow for any variations from anatomical norms during insertion and in no case should the instrument be forced against digitally felt resistance.
If passage of the Pipet Curet™ through the cervical canal is not found to be easily achievable, the instrument should not be forced and the possibility of the presence of pathologic cervical stenosis considered. With elderly patients in whom an extremely dry cervix may cause resistance to the instrument’s passage, very slight lubrication of the sheath with a sterile water soluble gel may facilitate its insertion.
ADVERSE REACTIONS
The following adverse reactions have been occasionally suspected or reported. The order of listing does not indicate frequency or severity.
- Injury to uterus (perforation)
- Cramping
- Uterine spasm
DIRECTIONS FOR USE
1. Prepare the vagina and cervix using currently accepted antiseptic techniques as you would for any intrauterine procedure.
2. With the vaginal speculum in place and open to expose the uterine cervix, gently probe the uterus for both its depth and direction with a uterine sound. DO NOT USE the Pipet Curet™ as a uterine sound. Then grasp the cervix with a very fine forceps or a tenaculum. If the uterus is anteverted, this grasp should be applied to the anterior lip of the cervix. If the uterus is retroverted, the grasp should be applied to the posterior lip of the cervix.
If the uterus is normally positioned and the cervix is stable, it is possible that the use of forceps or a tenaculum may not be necessary.
3. Now withdraw the speculum approximately 2 cm and apply gentle traction to the forceps or tenaculum to straighten any cervical curvature and to stabilize the cervix.
4. With the piston positioned at the extreme distal end of the sheath, the Pipet Curet™ is then inserted into and gently passed through the cervical canal and into the cavity of the uterus to a depth that corresponds to that which was determined by uterine depth finding (Figure 1). Slight friction can usually be felt with the fingers as the Pipet Curet™ passes through the internal cervical OS. IN NO EVENT SHOULD FORCE BE USED to obtain passage if resistance is encountered. Slight lubrication of the sheath with a sterile water soluble gel may facilitate its passage in patients with an extremely dry or narrow cervical canal. If, as is usually not the case, negotiation of the cervical canal proves painful, brief topical use of an anaesthetic agent may help facilitate introduction of the Pipet Curet™.

5. When the sheath is in position within the uterine cavity, discontinue any traction you have applied with a tenaculum of forceps. Then, while holding the sheath in position with one hand, with the other hand rapidly pull the piston firmly and without interruption (with one swift steady motion) toward the proximal end of the sheath as far as it will go (Figure 2).

NOTE: Slow interrupted or partial withdrawal of the piston will not produce the amount of negative pressure (suction) necessary to obtain the maximum tissue biopsy. An indentation in the wall of the sheath will prevent total withdrawal of the piston from within the sheath. This action creates a negative pressure (suction) within the sheath that draws the tissue into the curette opening at the distal end of the sheath and captures the separated tissue within its lumen.
6. Immediately after pulling the piston the full permissible distance, the sheath should be continuously rotated 360° by rolling or twirling between the fingers while moving the sheath laterally and back and forth (in and out) between the fundus and internal OS at least 3 or 4 times to obtain sample. It should then be gently withdrawn from the uterus (Figure 3). Examination of the sheath should then reveal a specimen of the uterine mucosa of histologic quality clearly visible within the sheath. Bleeding, if it occurs at all, is usually minimal.

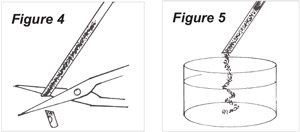
7. For histologic assessment of the specimen, the tip of the sheath should now be sectioned just proximal to its distal curette opening (Figure 4). The piston should then be advanced within the sheath to express the specimen from the sectioned sheath into an appropriate transport medium (Figure 5).
8. For bacterial culturing of the specimen, leave the piston in its fully withdrawn position and do not section the sheath at its distal curette opening. Immediately send the entire, intact instrument with the specimen captured within it to the laboratory with instructions to section the distal tip at a point at least 2 mm proximal to the distal curette opening and then to express the sample by use of the piston onto the appropriate culturing medium. Alternatively, immediately following biopsy, section the sheath just proximal to the distal curette opening *- then, by advancing the piston, express the sample onto appropriate medium in a transport container and send it to the laboratory for culturing.


